Remote Wheelchair Prescription: Initial System Evaluation
Andi Saptono, MS, Richard Schein, MS, Bambang Parmanto, PhD and David Brienza, PhD
RERC on Telerehabilitation, University of Pittsburgh, Pittsburgh, PA 15260
ABSTRACT
We present an initial evaluation of a remote wheelchair prescription system. In our previous work, we presented the design of the information technology infrastructure to support various projects within the Rehabilitation Engineering Research Center (RERC) on Telerehabilitation. In this paper, we evaluate the system used to support the remote wheelchair teleassessment. The teleassessment was conducted at a rural medical center, located about 100 miles away from the RERC. The rural medical center team was able to clearly communicate with the expert therapist from the RERC. We have confidence that the system is extensible across other telerehabilitation areas.
Keywords:
telerehabilitation; teleassessment; wheelchair; information technology; evaluation
BACKGROUND
The quality of the service delivered in a telerehabilitation setting depends on the media chosen for building the technology infrastructure (1). Our previous report had presented the design of the technological infrastructure to support a virtual team in assessing the client's need in a remote wheelchair prescription activity. One of the main guiding principles used in the RERC Telerehabilitation was that the technology is based on the Internet protocol, is cost-effective -utilizing components from open source initiative as necessary, and is intuitive to use.
Previous studies on the remote wheelchair prescription assisted us to identify and formulate the features needed by the virtual team, including: the need to use teleassessment to expand and support the local therapist by involving a remote therapist (2); the need to have the session meet a certain standard of practice by having an expert therapist join the assessment; the need of higher clarity visual streaming to have a higher quality of direct evaluations by the remote therapist (1); the need to communicate securely for privacy and confidentiality; and the need of archiving to review the sessions. In addition to this synchronous, active communication collaboration needs, the virtual team also need an asynchronous system to help them manage the information acquired (3).
Therefore, our next step is to ensure that the technology implemented matches the needs of the telerehabilitation setting. This report describes our evaluation on the system which was used to support a remote wheelchair assessment session. The case study, however, is a part of our initial study and, therefore, is used mainly to illustrate the obstacles, solutions, and possible future advancements of the project.
METHODS
The wheelchair teleassessment utilized a low-cost multipoint web conferencing system. We use ConferenceXP which offers a low-cost solution to support our virtual team. In order to test the visual quality of the system, we evaluated several web cameras, including: Creative Labs Webcam Live!, Logitech Quickcam for Notebook, and Logitech Orbits MX. We also tested a number of microphones (such as the USB microphone) for capturing the audio in addition to the camera's built-in microphone. All of these cameras have a price range below $200, in line with our goal for incurring minimal costs on all participants. The complete system specification to support the conferencing system is presented in Table 1.
| Infrastructure - Server Site | ||||
|---|---|---|---|---|
| Venue Server | Archive Server | Online Portal Server | Reflector Server | |
| Computer Type | Xeon 3GHz with 6GB memory | PIII 1GHz with 1.5GB memory | ||
| Harddisk capacity of 400GB * | ||||
| Connection Type | T1 Connection ** | |||
| Application Needed | Venue Service | Archive Service | SharePoint | Reflector Service |
| SQL Server 2005 | ||||
| User Sites | ||||
| Rural Clinic Site | Expert Therapist Site | |||
| Computer Type | At least PIV 3GHz with 512MB memory | At least PIV 3GHz with 512MB memory | ||
| Connection Type | Commercial DSL Line | T1 Connection | ||
| 5MB/728KBps | ||||
| Application Needed | ConferenceXP Client | ConferenceXP Client | ||
| Visual System | Logitech Orbit MX | Logitech Orbit MX | ||
| Sound system | Integrated Microphone | USB Microphone | ||
| External Speaker | External Speaker | |||
| * The online portal, venue service, and the archive service are installed in the same machine ** All infrastructure services are installed in the same network |
||||
The teleconferencing system allows for a synchronous communication between the therapists at the rural hospital and experts at the University of Pittsburgh Medical Center (UPMC). This video communication is enriched with a multimodal information sharing capability of the system, including sharing of documents web browser, and of presentation. The system is supported by a database system capable of recording the teleassessment session. The recording can be retrieved later to assist the therapist to review the session. Deploying the system requires a minimal amount of effort to set up compared with high-end video conferencing solutions. The system employs a point-and-click interface to access most of its functions.
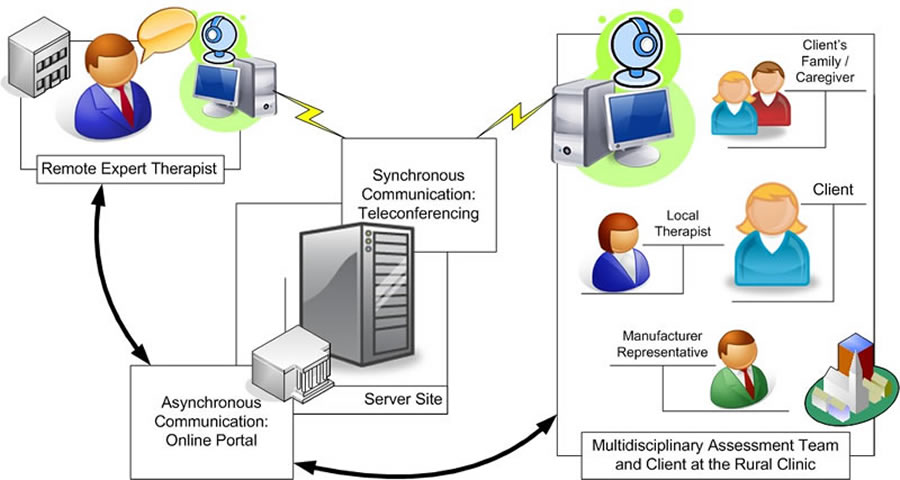 Figure 1. Teleasessment Communication Schema (Click image for larger view)
Figure 1. Teleasessment Communication Schema (Click image for larger view) To meet the need for an asynchronous communication system, we deployed an online collaboration portal. The online portal provides a way to share textual information, such as documents and survey results, and non-textual information, such as multimedia files. The online portal is designed to be modular and can be tailored easily. For example, within the portal, online forms can be created to collect data from multiple sites and a summary of therapy results can be produced for both the therapist and the client. The online portal serves as the information integrator to support the interaction between therapists, the client, and the client's family.
The following is the illustration of the technological infrastructure design to support the remote wheelchair prescription system. Figure 1 illustrates the interaction flow of the virtual teams that includes the rural multidisciplinary team and remote experts, supported by the synchronous and the asynchronous communication system.
EVALUATION
We conducted our pilot study by connecting Dubois Regional Medical Center (DRMC) in rural Dubois (PA) with UPMC in Pittsburgh (PA). The two facilities are about 100 miles apart. A web camera (Logitech Orbit MX) was sent and installed on a computer in the wheelchair assessment clinic at DRMC. The clinic at DRMC is connected to the Internet by a wireless connection and by a DSL line with a downstream bandwidth of 5 Mbps and an upstream bandwidth of 728 Mbps. Installing ConferenceXP software at DRMC did not present any problem. We did, however, encounter problems connecting the video conferencing system due to network and firewall issues. The wireless connection was too slow for the video conferencing system. This problem was solved by connecting the computer directly to a DSL line. Another problem was the strict firewall setting at both sides (UPMC and DRMC). The strict firewall setting is common in health care institutions. ConferenceXP needs a specific path to be opened in the firewall system to allow communication with other peers on the network. The firewall problem was solved by opening five ports in the firewall system.
We did not encounter any difficulty in directing DRMC's therapists. The system's point-and-click interface is relatively intuitive for the therapist to understand without a training session. The remote therapist at DRMC and the expert at UPMC reviewed the system thoroughly by going over a requirements check list before conducting the real wheelchair assessment with the client. The archiving feature was also tested prior to the actual assessment session.
The teleassessment was done with a multidisciplinary team that included the client, the client’s family member(s)/caregiver, local therapists, assistive technology suppliers, manufacturer representatives and remote expert therapists. The remote expert therapist agreed that our implementation of the conferencing system delivered an ideal video and audio quality for the teleassessment. The expert therapist was able to monitor the therapy session in a real time, ask necessary questions, and get responses in a timely manner. An abundance amount of communication went back and forth, and the virtual team was able to have a good flow on the assessment session. We also found that talking clearly and slowly increased the clarity of the communication. The DSL connection line dropped several time during the session but it did not hinder the assessment session as the problem can be fixed almost immediately (took less than a minute to rejoin the conference).
FUTURE WORK
The current limitations of the solution include the lack of remote control over the camera and the limit of the bandwidth size. The lack of control over the remote camera was mitigated by manual control of the camera by the remote site’s therapists. We are looking for a solution that will allow the experts to remotely control the camera view during the teleassessment. A possible solution is to employ multiple angle cameras or to place an additional network camera. The quality of this solution, however, depends on the size of the bandwidth available. To properly deploy this solution, a higher bandwidth size is needed to stream all video and audio data over the network, which will translate into a higher, more costly communication channel.
Our next step is to deploy the system at Charles Cole Memorial Hospital located in Coudersport, PA. We are also looking to deploy the system around other places surrounding the city of Pittsburgh. We believe the modular infrastructure will be helpful across other telerehabilitation areas to further improve health service delivery over the distance.
REFERENCES
- Malagodi M., Schmeler M.R., Shapcott N.G., Pelleschi T. (1998). The use of Telemedicine in Assistive Technology Service Delivery: Results of a Pilot Study. Technology: Special Interest Section Quarterly, 8(1), 1-4.
- Burns RB, Crislip D, Daviou P, Temkin A, Vesmarovich S, Anshutz J, Furbish C, and Jones ML. (1998). Using Telerehabilitation to Support Assistive Technology. Assistive Technology, 10, 126-133
- Winters, J.M. (2002). Telerehabilitation Research: Emerging Opportunities. Annu Rev Biomed Eng., 4, 287-320.
CORRESPONDENCE
Andi Saptono, M.S.
6025 Forbes Tower,
School of Health and Rehabilitation Sciences
University of Pittsburgh
Pittsburgh, PA 15260.
(412) 383 5101.
ans38@pitt.edu.
Highlights
- Source Ordered
- No Tables
- Very Compatible
Gargoyles
Disney produced a television show in the mid 1990s called Gargoyles. It's a great show and I'm a big fan. A few years ago Disney started to release the show on DVD. The last release was of season 2, volume 1. That was two years ago. Volume 2 has not been released. Why? Poor sales. So if you should find yourself wanting to support my work, instead I ask you pick up a copy of season 2, volume 1. It's a great show and you might find yourself enjoying it.