Development of a Community Mobility Skills Course for Persons Who Use Mobility Devices
Kimberly A. Walker, OTDS, David B. Gray, PhD, Holly Hollingsworth, PhD, Kerri Morgan, MSOT, OTR/L, Keri DeGroot, OTDS
ABSTRACT
A community mobility skills course (CMSC) was developed to assess an individual’s mobility device skills in the ‘lived-in’ environment and relate them to their skills in a ‘controlled’ environment as measured by an inside mobility skills course (IMSC). Once designed the CMSC was piloted by four individuals using mobility devices within four mobility device groups (cane/crutch/walker, manual wheelchair, power wheelchair, or scooter). The purposes of the CMSC were to assess and relate an individual’s mobility device skills in the ‘lived-in’ environment, to determine if an IMSC adequately prepares people for use of their devices in the ‘lived-in’ environment, and to determine what environmental factors may be unique to community mobility and are not tested in a clinical environment.
KEYWORDS:
mobility device, assessment, community mobility, skills course
STATEMENT OF PROBLEM
Rehabilitation scientists have recognized the need for testing mobility device skills in the ‘lived-in’ natural environment but most are currently testing mobility device skills only in the ‘controlled’ clinical environment.
BACKGROUND
According to Kaye, Kang, and LaPlante [(1)] over 6.8 million Americans use assistive devices to help them with mobility. Out of this group 1.7 million use some type of wheelchair or scooter while 6.1 million (2.4 percent of the population) use a device such as canes, crutches, or walkers [(1)]. For a person in a wheelchair to function independently, they must possess a variety of skills that will help them to overcome physical barriers found in the environment; training of these skills is a vital part of the rehabilitation process [(2)]. According to MacPhee, Kirby, Coolen, Smith, Macleod, & Dupuis, [(3)] few rehabilitation programs have focused on the training of mobility device skills even though evidence suggests that training could improve independence, freedom of movement, and quality of life. Evidence suggests that rehabilitation is more effective when provided in the client’s own environment and the goal is to achieve re-integration into the client’s community [(4)]. According to Wade [(4)] some evidence indicates that clinical settings are more conducive to interventions because the environment is better in the clinic. However, these clinical settings are less relevant to the client, may not be used by the client after discharge from rehabilitation and may not generalize to use in the community [(4)].
One example of a measure used to identify a wheelchair user’s skills in a safe and controlled environment is the Wheelchair Skills Test (WST) [(5)]. The WST documents initial status and subsequent improvements for wheelchair users, provides an outcome measure for rehabilitation programs, assists in testing research hypotheses, and is used to assist in the development of new technologies [(5)]. The WST is an objective measure that is used to assess wheelchair function at the level of detail that corresponds to daily life [(6)]. A brief, formalized period of wheelchair skills training using the WST did significantly improve wheelchair skills [(3)].
One of the limitations in the current mobility device skills evaluation studies is that they do not evaluate mobility device skills in the ‘lived-in’ environment. Another limitation of these studies is that they only assess power and manual wheelchairs and do not include other types of assistive devices such as scooters and canes, crutches, and walkers. The purpose of this project was to develop and pilot a mobility device skills assessment protocol in the community that is specific to the type of device used (i.e. power wheelchair, manual wheelchair, scooter, and cane/crutches/walker).
METHODS
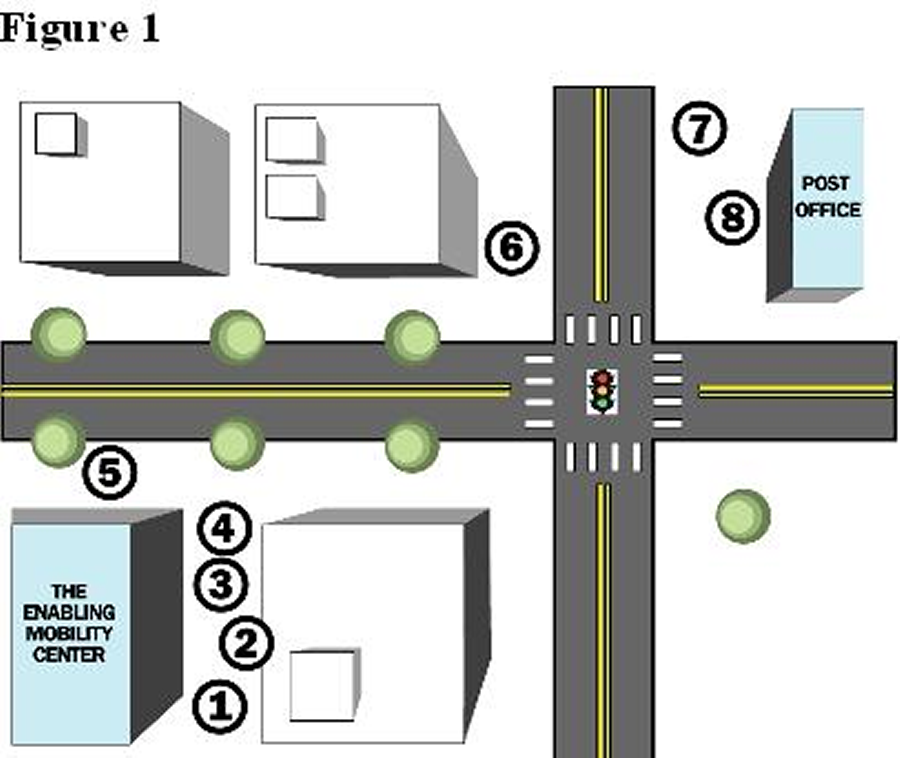 Figure 1. d (Click image for larger view)
Figure 1. d (Click image for larger view) The CMSC was developed to identify mobility skills strengths and weaknesses of persons who use mobility devices in the ‘lived-in’ environment. The CMSC design and protocol is based on the Wheelchair Skills Test (WST) protocol developed by Dr. Lee Kirby for manual wheelchair users and the IMSC protocol developed by Dr. David B. Gray and colleagues for four mobility device groups (power wheelchair, manual wheelchair, scooters, and cane/crutches/walker). The CMSC was designed in the community of University City, Missouri (See Figure 1). The nine tasks included on the course are: opening and closing a door, level driving and walking in both forward and reverse directions, moving turns commonly referred to as a figure 8 design, turning in place both in the right and left directions, moving on a cross slope with both a right and left slope, going up and down curbs of 1.5 and 2 inches, driving or walking over uneven terrain, driving or walking up and down an incline, walking up and down 2 stairs (this task was only completed by individuals who use a cane/crutch/walker).
Participants
 Figure 2. d (Click image for larger view)
Figure 2. d (Click image for larger view) Four participants were selected from a sample of 91 adults who completed the IMSC, the Assistive Technology CORE Survey (which measures demographics, general health and wellness, assistive technology use, transportation use and current participation in exercise) and the Community Participation and Perceived Receptivity Survey or CPPRS (which measures the frequency and quality of participation across sites in the community). They ranged in age from 18 – 80, included both men and women, and had a mobility impairment that required the use of a mobility device (cane/crutch/walker, manual wheelchair, power wheelchair, or scooter). All participants lived in the community and had been discharged from rehabilitation for at least one year at the time of study. The IMSC sample included 43 persons who used a power wheelchair, 24 who used a manual wheelchair, 14 who used a scooter and 10 who used a cane, crutch, or walker. The selection of the four participants for the CMSC was based on having one individual from each of the four device groups (cane/crutch/walker, manual wheelchair, power wheelchair, or scooter).
Materials
Each device group has an evaluation form that is completed by a trained staff member, which includes a variety of tasks completed at a person’s skill level. Each task included on the evaluation form is scored on completion, safety, time, and task instruction. Completion is scored on a 4 point scale with a score of 4 indicating that the participant completed the task with no assistance from the evaluator (i.e. verbal or physical). If a participant is unable to complete a task the participant is given a score of 1. Safety is also scored on a 4 point scale, with a score of 4 indicating that the participant completed the task safely. A score of 1 indicates a maximum safety risk or that the evaluator had to intervene to prevent injury. Time taken is the amount of time in seconds that a participant requires to complete a task. Task instruction is also scored on a 4 point scale with a score of 4 indicating instructions were clearly provided by the participant to complete the task. A score of 1 indicates the participant was unable to give any instruction about how to complete the task.
Procedures
The Washington University human subjects committee approved all procedures. After obtaining informed consent, participants were evaluated on the CMSC provided at the Enabling Mobility Center through the Washington University Program in Occupational Therapy and Paraquad (an Independent Living Center). Participants were asked to perform a series of tasks on the course and were scored on their performance. During the completion of each task, each participant was carefully monitored by a member of the research team to ensure safety. Once the CMSC was completed the 4 individual time scores were compared to the mean time score of their device group on the IMSC and their performance on the inside course (IMSC). The mean time score for each device group on the IMSC was obtained using the time scores of the 91 participants from the previous study.
RESULTS
Participant #1 completed all timed tasks faster on the CMSC versus the IMSC (See Table 1). Participant #1 asked for assistance in completing the tasks of “opening a door toward” and “opening a door away” on the CMSC but completed the tasks independently on the IMSC. Participant #1 completed the task of going up a 1.5 inch curb on the IMSC but refused to attempt the task on the CMSC. Times on both the IMSC and CMSC were faster than the mean of power wheelchair users on the IMSC.
| Task | IMSC Group | IMSC Individual | CMSC Individual |
|---|---|---|---|
| Level Driving | 11 |
10.1 |
4.1 |
| Driving in Reverse | 30.9 |
19.4 |
5.7 |
| Moving Turns | 36.9 |
20.1 |
13.5 |
| Turns in Place (left) | 9.3 |
20.1 |
13.5 |
| Turns in Place (right) | 7.2 |
2.6 |
2.1 |
| Cross Slope (left) | 12.3 |
11.6 |
6.3 |
| Cross Slope (right) | 9.4 |
13.7 |
5.6 |
| Carpet/Grass | 13.4 |
13.4 |
10.9 |
| Going UP Incline | 16.9 |
12.4 |
7 |
| Going DOWN Incline | 17.6 |
16 |
6.5 |
| UP Curb (1.5") | 9.3 |
4.1 |
md* |
| DOWN Curb (1.5") | 6.4 |
8.5 |
1.1 |
| md = missing data, performance is documented as time in seconds | |||
Participant #2 completed some of the timed tasks (level propelling forward, moving turns, going across a cross slope and going up and down a 1.5 inch curb) faster on the CMSC versus the IMSC (See Table 2). Participant required minimal physical assistance to propel up the incline on the IMSC. On the CMSC participant #2 attempted to open the door (away) independently and was unable to complete, he was then prompted by the evaluator to ask for help and then was able to give the evaluator instructions to open the door. While going down the incline on the CMSC the participant ran into the handrail on the right side. Participant #2 refused to attempt the two inch curb and the uneven terrain (grass) on the CMSC. Participant #2 was slower than the mean time for manual wheelchair users on tasks such as moving turns, turns in place, cross slope, and curbs completed on the IMSC.
| Task | IMSC Group | IMSC Individual | CMSC Individual |
|---|---|---|---|
| Level Driving | 16.3 |
11.2 |
8.4 |
| Driving in Reverse | md* |
md |
12.4 |
| Moving Turns | 32.5 |
44.2 |
26.1 |
| Turns in Place (left) | 9.7 |
11 |
11.6 |
| Turns in Place (right) | 6.5 |
7.4 |
10.1 |
| Cross Slope (left) | 17.1 |
32.1 |
14.6 |
| Cross Slope (right) | 13.4 |
30.8 |
14.8 |
| Carpet/Grass | 21.6 |
16.6 |
md |
| Going UP Incline | 27 |
22.9 |
39 |
| Going DOWN Incline | 16.8 |
14.8 |
30.3 |
| UP Curb (1.5") | 6.3 |
9.1 |
8.6 |
| DOWN Curb (1.5") | 3.7 |
5.1 |
4.5 |
| md = missing data, performance is documented as time in seconds | |||
Participant #3 completed most of the timed tasks faster on the CMSC versus the IMSC, with the exception of cross slope right and going down a 1.5 inch curb (See Table 3). The participant completed all of the same tasks on the CMSC as she did on the IMSC. On the IMSC participant #3 was slower than the mean for scooter users on the tasks of level driving in both directions, moving turns, turning in place right, cross slope left, and going up and down an incline.
| Task | IMSC Group | IMSC Individual | CMSC Individual |
|---|---|---|---|
| Level Driving | 13 |
13.7 |
3.4 |
| Driving in Reverse | 24.5 |
29.8 |
8.9 |
| Moving Turns | 23 |
26.3 |
10.2 |
| Turns in Place (left) | 23.7 |
20.5 |
12.4 |
| Turns in Place (right) | 19 |
23.3 |
12.4 |
| Cross Slope (left) | 8.7 |
10.6 |
6.4 |
| Cross Slope (right) | 9.2 |
6.4 |
9.6 |
| Carpet/Grass | 11 |
9.2 |
9.2 |
| Going UP Incline | 10.4 |
12.4 |
9.1 |
| Going DOWN Incline | 13.8 |
14.4 |
11.6 |
| UP Curb (1.5") | 2.9 |
3.1 |
1.5 |
| DOWN Curb (1.5") | 5.5 |
2.5 |
2.7 |
| Performance is documented as time in seconds | |||
Participant #4 completed timed tasks such as moving turns, going up and down a 1.5 inch curb, going up and down stairs, and going up an incline faster on the CMSC versus the IMSC (See Table 4). Participant #4 completed timed tasks such as left and right turns in place, uneven terrain (grass), and going down an incline slower on the CMSC versus the IMSC. Participant #4’s times are only faster than the mean of cane, crutch, and walker users on the IMSC task of uneven terrain (carpet).
| Task | IMSC Group | IMSC Individual | CMSC Individual |
|---|---|---|---|
| Level Driving | 15.4 |
md* |
1.6 |
| Driving in Reverse | 44.4 |
md |
37 |
| Moving Turns | 21.2 |
26.2 |
24.7 |
| Turns in Place (left) | 3.2 |
1.4 |
3.9 |
| Turns in Place (right) | 4.3 |
3.9 |
4.3 |
| Cross Slope (left) | 11.1 |
md |
15.6 |
| Cross Slope (right) | 10.9 |
md |
10.6 |
| Carpet/Grass | 18.4 |
14.4 |
27.1 |
| Going UP Incline | 18.5 |
18.7 |
18.5 |
| Going DOWN Incline | 19.1 |
21.3 |
26.2 |
| UP Curb (1.5") | 3.9 |
3 |
1.6 |
| DOWN Curb (1.5") | 3.2 |
4.6 |
3.5 |
| md = missing data, performance is documented as time in seconds | |||
DISCUSSION
When comparing the IMSC scores to the CMSC scores several of the participants completed the CMSC tasks faster. A reason for this may be that learning occurred as the participants completed the IMSC since all participants did this course first and then the CMSC. This could be controlled in future research by counter balancing the participants. Another possible reason is that the outside environment contains more open space with less threat of running into walls or furniture and therefore the participants may not have been as careful with their device use. This study demonstrated differences in performances of tasks in the clinical (IMSC) and community (CMSC) settings by all four mobility device users. Further research is needed to determine if these differences hold for groups of mobility device users and to discover the factors linked to these differences. The value of this study is that when the individual scores of mobility device users are below the mean of their device group scores, then they may benefit from mobility device training. The next phase of this type of research, using a larger sample, could provide useful information for studying the generalization of mobility skills taught in clinical settings to improved performance in the community. With this study we developed a CMSC that is feasible and easy to use. The assessment requires no costly equipment, takes a short amount of time to complete, and should be simple to duplicate in other community environments. The CMSC may provide a tool that will improve safe and efficient use of mobility devices. The improved performance using mobility devices may have some positive influence on increasing community participation of people with lower limb impairments and mobility limitations and lead to a decreased risk of isolation.
REFERENCES
- Kaye, H. S., Kang, T., LaPlante, M.P. (2000). Mobility device use in the United States (No. 14). Washington: U.S. Department of Education, National Institute on Disability and Rehabilitation Research.
- Kilkens, O. J., Dallmeijer, A. J., de Witte, L. P., van der Woude, L. H., & Post, M. W. (2004). The Wheelchair Circuit: Construct validity and responsiveness of a test to assess manual wheelchair mobility in persons with spinal cord injury. Archives of Physical Medicine and Rehabilitation, 85, 424-431.
- MacPhee, A. H., Kirby, R. L., Coolen, A. L., Smith, C., MacLeod, D. A., & Dupuis, D. J. (2004). Wheelchair skills training program: A randomized clinical trial of wheelchair users undergoing initial rehabilitation. Archives of Physical Medicine and Rehabilitation, 85, 41-50.
- Wade, D. T. (2003). Community rehabilitation, or rehabilitation in the community? Disability and Rehabilitation, 25(15), 875-881.
- Kirby, R. L., Swuste, J., Dupuis, D. J., MacLeod, D. A., Monroe, R. (2002). The wheelchair skills test: A pilot study of a new outcome measure. Archives of Physical Medicine and Rehabilitation, 83(1), 10-18.
- 6. Kirby, R. L., Dupuis, D. J., MacPhee, A. H., Coolen, A. L., Smith, C., Best, K. L., Newton, A. M., Mountain, A. D., MacLeod, D. A., Bonaparte, J. P. (2004). The wheelchair skills test (version 2.4): Measurement properties. Archives of Physical Medicine and Rehabilitation, 85(5), 794-804
ACKNOWLEDGEMENT
This study was funded by the National Institute on Disability and Rehabilitation Research.
This project was supported by the following persons: Sue Tucker, MSOT OTR/L, Carla Walker MSOT OTR/L, Jessica Dashner OTD OTR/L, Melissa Lyles, MSOT OTR/L, Polly Gray, and Denise Curl.
AUTHOR CONTACT INFORMATION
Kimberly A. Walker, OTDS
Paraquad, ILC
5240 Oakland Ave
St. Louis, MO 63110
Voice: (314)289-4344
Fax: (314)289-4201
Email: kwalker@paraquad.org
Highlights
- Source Ordered
- No Tables
- Very Compatible
Gargoyles
Disney produced a television show in the mid 1990s called Gargoyles. It's a great show and I'm a big fan. A few years ago Disney started to release the show on DVD. The last release was of season 2, volume 1. That was two years ago. Volume 2 has not been released. Why? Poor sales. So if you should find yourself wanting to support my work, instead I ask you pick up a copy of season 2, volume 1. It's a great show and you might find yourself enjoying it.