A System to Detect Motion in the Sagittal Plane
Blair A. Rowley, Ph.D., and Amy R. Bierce, M.S.
Wright State University,
Dayton, Ohio
ABSTRACT
Unintentional falls were responsible for 5.5% of all deaths in the United States in 2001. There are countless causes for falls, many of which are due to age or medical conditions. It is unknown whether there are any motion indicators that a patient is unstable just before falling. This paper describes the design of an instrument that can detect perturbations in posture and may be useful in clinical trials to determine if any vibrations, shaking, or swaying occur just prior to a patient’s fall. The device counted how many times perturbations occurred using an electro-mechanical system. A microprocessor program was developed to detect motion that was unlikely to be due to normal activities. Trials were conducted on a healthy subject. The instrument used a single axis sensor for proof of concept.
KEY WORDS:
falling; gyroscope; microprocessor; motion detection; Progressive Supranuclear Palsy.
PURPOSE
There are many reasons older people lose their balance and fall down. Known causes for falls include syncope, dizziness, orthostasis, instability, sensory deficit, illness, age-related frailty, and medication (1). Patients with early symptoms of a disease called Progressive Supranuclear Palsy, experience a loss of balance or stability, which can lead to falls. In this disease, symptoms become progressively worse over time. As with many diseases, there are medications available that may help patients with some of the symptoms (2). However, the exact cause of a falling incident is not always known.
According to the National Safety Council, of 39,389,000 injury-related emergency room visits in 2001, 7,762,000 were due to falls (3). Unintentional falls accounted for 5.5% of all deaths in the United States in 2001 (4). The number of deaths due to falls, increases with age and accounts for one third of all unintentional-injury deaths of the elderly (5).
Presently, it is unknown whether there are any measurable warning signs just before a patient falls. Potential indicators may be patient sways, shakes, or vibrations. Thus, it would be advantageous to have a way of measuring how many times a patient sways or shakes, in comparison to a healthy individual. Perhaps once this is known, a motion-sensing device can be adapted to send out a warning signal to patients when a fall seems imminent so that they may brace themselves and reduce or eliminate the fall.
The purpose of this project was to design and construct an instrument that could detect motion in the sagittal plane and separate normal background motion from motion of interest.
METHODS
 Figure
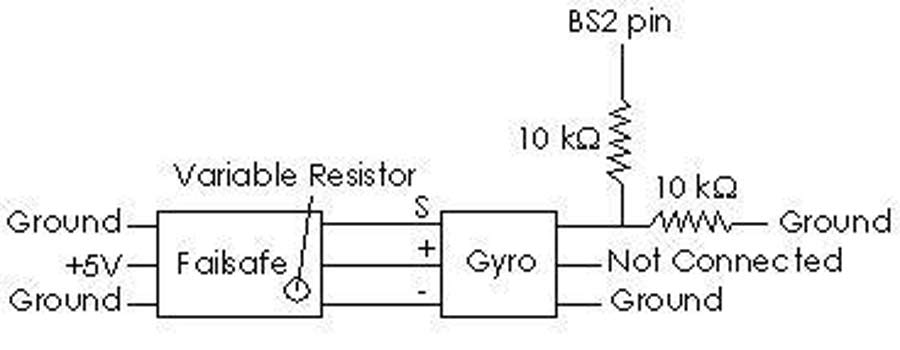
1 - The basic design of the hardware is shown here. The failsafe generated
pulses every 20.5 ms that were 1.5 ms wide. The gyro then modified the
pulse width up to +/- 0.25 ms. This pulse served as input to a Basic Stamp
port. (Click image for larger view)
Figure
1 - The basic design of the hardware is shown here. The failsafe generated
pulses every 20.5 ms that were 1.5 ms wide. The gyro then modified the
pulse width up to +/- 0.25 ms. This pulse served as input to a Basic Stamp
port. (Click image for larger view) Motion detection can be achieved through the use of an electro-mechanical sensor, such as a gyroscope. For this system, a gyroscope was used to detect motion in the sagittal plane. It has been shown by others that gyroscopes produce data that correlates well with that of video tracking methods (6, 7, 8, 9, 10). In this system the gyroscope output was measured by a microprocessor. The extreme and normal values ignored, and the applicable or unusual values counted. The microprocessor program was designed to detect motion that occurred beyond normal movement and before falling. For the purpose of this paper this region was called the symptomatic zone. The output of the program can be stored and later sent to a PC for interpretation. For proof of concept this instrument used a single axial sensor.
A. Instrument Hardware
There were three main components: a JR/HITEC single channel electronic failsafe (#362), a GWS Piezo Gyroscope (model PG-03), and a BASIC Stamp microprocessor (BS2). The failsafe and gyroscope are typically found in remote controlled model airplanes. In model airplanes, the gyroscope input comes from the receiver, which is in series with the failsafe. If the receiver signal is lost, the failsafe produces and transmits a fixed signal to the gyroscope. The gyroscope then modifies and sends the signal to a servo which maintains the airplane’s position in the case of perturbations caused by wind gusts, etc.
 Figure
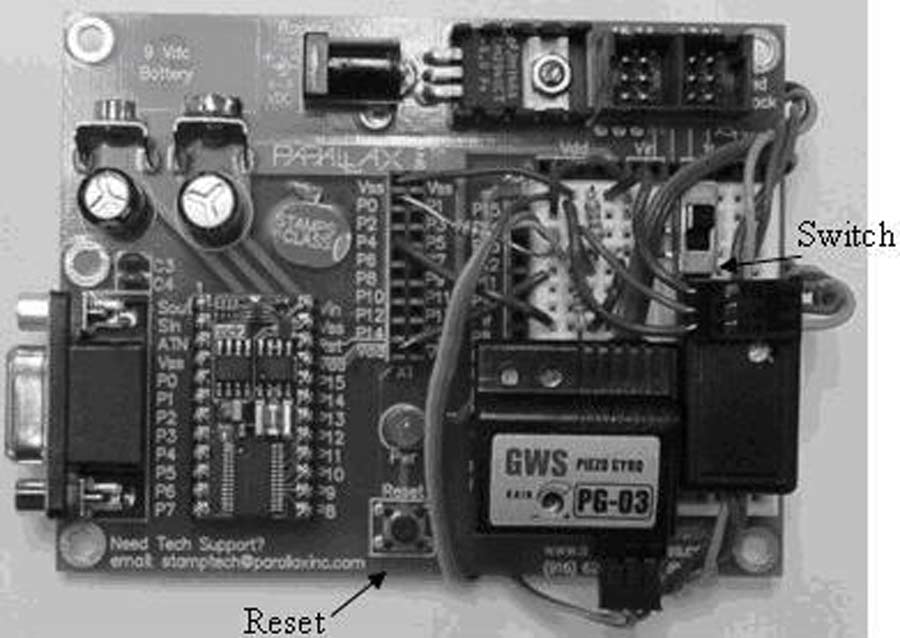
2 - The complete instrument used to detect motion is shown here. When the
reset button was pressed, previously stored data was erased and the program
measured how far the gyroscope had moved from neutral. The Basic Stamp generated
a count that was proportional to the pulse width. This cycle repeated until
the switch shown on the breadboard was moved to the “off” position.
(Click image for larger view)
Figure
2 - The complete instrument used to detect motion is shown here. When the
reset button was pressed, previously stored data was erased and the program
measured how far the gyroscope had moved from neutral. The Basic Stamp generated
a count that was proportional to the pulse width. This cycle repeated until
the switch shown on the breadboard was moved to the “off” position.
(Click image for larger view) The failsafe’s inputs were: receiver signal, power, ground, and a potentiometer. Its outputs were: control signal, power, and ground. Grounding the failsafe’s signal input caused it to produce a fixed output pulse with a period of 20.5 milliseconds. The potentiometer allowed adjustment of the pulse width, which was set to 1.5 milliseconds.
When the gyroscope detected motion, it modified the output pulse width up to +/- 0.25 milliseconds. The pulse width fluctuations were directly proportional to how far the gyroscope had moved from neutral. The gyroscope’s output signal served as the input to the microprocessor as shown in Figure 1.
B. Instrument Software
The BASIC Stamp program detected, analyzed, and stored motion data. The data was then uploaded to a PC at the completion of a trial.
The input to the Stamp program was electrical pulses with widths dependent upon how far the subject strayed from a stable position. The program measured the width of the pulse using an internal counter and then stored each count.
A reset button was pressed to clear old data, start the program, and begin data collection. Stopping the program, while retaining stored data, was accomplished with a switch that provided an input to another port on the Stamp. The switch was in the “on” position when the reset button was pressed, enabling data collection. When the switch was moved to the “off” position, the program stopped. The Stamp’s serial port allowed it to be connected to a PC and data uploaded (11).
 Figure
3 - The instrument was mounted on a top hat, which was chosen as an easily
wearable instrument support for trials. (Click image for larger view)
Figure
3 - The instrument was mounted on a top hat, which was chosen as an easily
wearable instrument support for trials. (Click image for larger view) An analysis was done using PBASIC’s memory map function to ensure stored values did not overwrite portions of the program. The Stamp could measure pulse widths from 2 microseconds to 0.13107 seconds. The pulse from the failsafe had a width of 1.5 milliseconds, thus it was detectable. The Stamp executed approximately 4000 instructions/second (12). The code for the program had 22 instructions. Therefore, the program would look for a new pulse every 5.5 milliseconds. Since the pulses were generated every 20.5 milliseconds the program would detect all of them.
C. Assembly of the Unit
All components were mounted on the Stamp’s Board of Education, as shown in Figure 2. A top hat was used to provide a flat surface that was easily wearable for trials, as shown in Figure 3. The Board of Education was affixed so that the gyroscope was horizontal with the axis of rotation parallel to a line that passed through a subject’s ears. In this position it would detect rotation in the sagittal plane.
D. Experimental Protocol
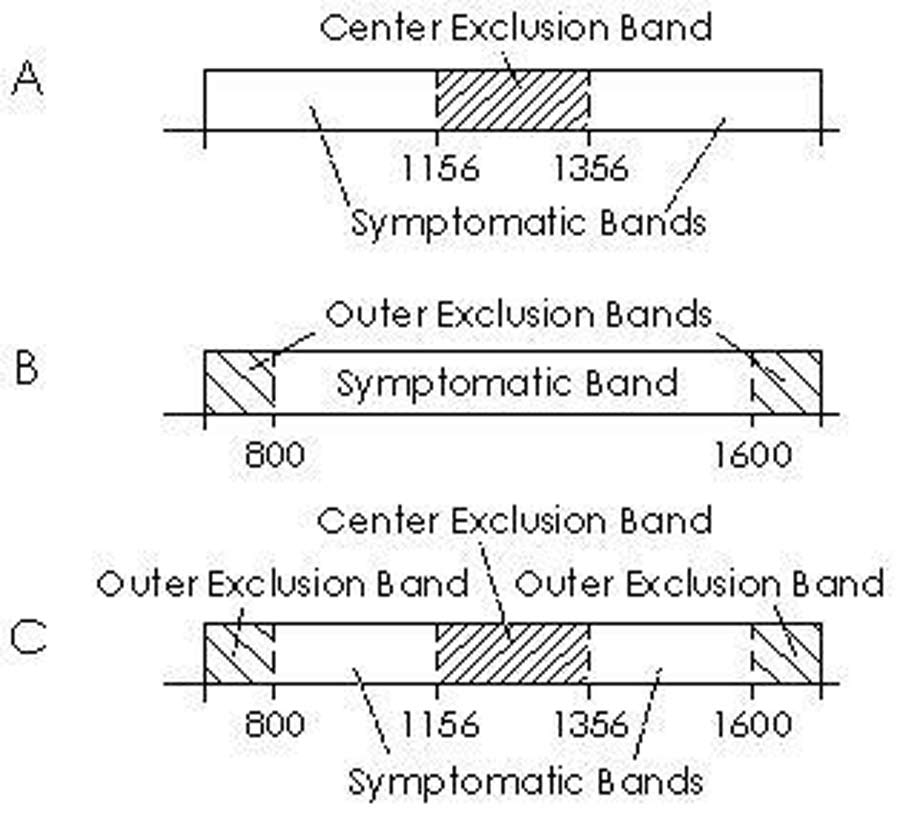
Measurements on the test subject showed normal counts ranging from 1156 to 1356. Sudden rotational motions fore and aft produced counts less than 800 and more than 1600. Based on these values, exclusion bands were created in the microprocessor program to evaluate data and eliminate counts due to normal motion and falling. Three sets of the exclusion bands were used: center exclusion band (A), outer exclusion bands (B), and using all exclusion bands (C), as illustrated in Figure 4.
Six trials were conducted during two common activities, walking on a flat surface and climbing stairs. Both activities were performed at a rate of 1 step/second and each trial was conducted within five minutes of another trial.
RESULTS
The results from the trials are shown in Table I.
| Trial number – activity |
Exclusion Bands Used |
Number of times motion is in Symptomatic Bands |
|---|---|---|
1 - walking |
A |
2,095 |
2 - walking |
B |
43,967 |
3 - walking |
C |
2,947 |
4 - stairs |
A |
667 |
5 - stairs |
B |
43,606 |
6 - stairs |
C |
4,643 |
DISCUSSION
 Figure
4 - The three sets of exclusion bands used in trials are shown here. Set
A used the center exclusion band, set B used the outer exclusion bands, and
set C used both the center and outer exclusion bands. (Click image for larger
view)
Figure
4 - The three sets of exclusion bands used in trials are shown here. Set
A used the center exclusion band, set B used the outer exclusion bands, and
set C used both the center and outer exclusion bands. (Click image for larger
view) A comparison of the data from the walking trials (1, 2, and 3) showed that most of the motion occurs in the center band. The data from trials 1 and 3 excluded the center band and had 95% and 93%, respectively, fewer counts than trial 2. This showed that the center band filtered out most normal walking counts. Trials 4, 5, and 6 show a similar pattern. In trial 6, the subject was becoming fatigued, which could be corrected by taking longer breaks between trials.
The number of counts in trials 1, 3, 4, and 6 may indicate that the center exclusion band was too narrow. Future research could also investigate the rate and patterns of symptomatic counts.
There was variability in the data due to small changes in walking pace and stair climbing. However, the data pattern was consistent for both cases. This variability could be reduced by using a treadmill and stair climber. Future trials could include patients with diseases that are known to cause falling, to determine if there is abnormal motion present during daily activities.
To the authors knowledge, similar published works have focused on degree of sway during quiet stance, sway amplitude and velocity, using force plates to measure change in center of gravity, qualitative functional balance testing, and sensory balance training (13, 14, 15). These testing methods are impractical for daily patient at-home monitoring. Sensory balance training has effectively reduced falls in patients with reduced or conflicting sensory inputs for a month after training.
CONCLUSION
A system for detecting and quantifying motion in the sagittal plane has been built and tested. The instrument could be expanded to detect multi-dimensional motion. Eventually, this may be used with patients to produce a sound, vibration, electrical stimulation, and/or light to warn of unstable posture prior to falling.
REFERENCES
- Injury Insights. (2002) National Safety Council. pp 6. [Online] http://www.nsc.org/email/june-july.pdf.
- Golbe, L. I. (1996). PSP Some Answers. Baltimore, MD: Society for Progressive Supranuclear Palsy. John Hopkins Outpatient Center.
- Advanced Data No. 335: Table 13. (2003) U.S. Department of Health and Human Services Center for Disease Control and Prevention. [Online] http://www.cdc.gov/nchs.fastats/pdf/ad335_t13.pdf.
- National Vital Statistic Reports: Deaths: Final Data 2001, (2003). U.S. Department of Health and Human Services Center for Disease Control and Prevention.[Online] http://www.cdc.gov/nchs/data/nvsr/nvsr52/nvsr52_03.pdf.
- Injury Facts. (2002). National Safety Council.
- Mayagoitia, R.E., Nene, A.V., and Veltink, P.H. (2002). Accelerometer and rate gyroscope measurement of kinematics: an inexpensive alternative to optical motion analysis systems. Journal of Biomechanics. 35. 537-542.
- Najafi, B., Aminian, K., Loew, F., Blanc, Y., and Robert, Ph. (2000). Falling Risk Evaluation in Elderly using miniature gyroscope. First Annual International IEEE- EMBS Special Topic Conference on Microtechnologies in Medicine & Biology. 557-561.
- Cappozzo, A. (1981). Analysis of the Linear Displacement of the Head and Trunk during Walking at Different Speeds. Journal of Biomechanics. 14. 6. 411-425.
- Kirtley, C., and Tong, K. (2000). Insole Gyro System for Gait Analysis. RESNA Conference Proceedings. Accessed May 24, 2006.
- Boonstra, M.C., van der Slikke, R.M.A., Keijsers, N.L.W., van Lummel, R.C., de Waal Malefijt, M.C., and Verdonschot, N. (2006). The accuracy of measuring kinematics of rising from a chair with accelerometers and gyroscopes. Journal of Biomechanics. 39. 354-358.
- BASIC Stamp Manual version 2.0. (2000). (Version 2.0b). Rocklin, CA: Parallax, Inc.
- Stamp FAQS: Functional Information. (2002). [Online]. http://www.parallaxinc.com/downloads/Documentation/Basic%20Stamps/stamp_faqs.pdf.
- Woollacott, M.H., and Shumway-Cook, A. (1997). Clinical and Research Methodology for the Study of Posture and Balance. In: Masdeu, J.C., Sudarsky L., and Wolfson, L. (1997). Gait Disorders of Aging: Falls and Therapeutic Strategies. Lippincott-Raven Publishers: Philadelphia.
- Woollacott, M.H., Moore, S., and Hu, M.H. (1993). Improvements in Balance in the Elderly Through Training in Sensory Organization Abilities. In: Stelmach, G.E., and Hömberg, V. (1993). Proceedings of the NATO Advanced Research Workshop on Sensorimotor Impairment in the Elderly. Klewer Academic Publishers: Boston.
- van Wegen, E.E.H., van Emmerik, R.E.A. and Riccio, G.E. (2001). Active Postural Sway and the Detection of Stability Boundaries. In: Burton, G. and Schmidt, R.C. (2001). Studies in Perception and Action VI, Eleventh International Conference on Perception and Action. Lawrence Erlbaum Associates Publishers: London.
Contact:
Blair A. Rowley
207 Russ Engineering Center
3640 Colonel Glenn Hwy.
Dayton, OH 45435
Highlights
- Source Ordered
- No Tables
- Very Compatible
Gargoyles
Disney produced a television show in the mid 1990s called Gargoyles. It's a great show and I'm a big fan. A few years ago Disney started to release the show on DVD. The last release was of season 2, volume 1. That was two years ago. Volume 2 has not been released. Why? Poor sales. So if you should find yourself wanting to support my work, instead I ask you pick up a copy of season 2, volume 1. It's a great show and you might find yourself enjoying it.